Interviewer: Welcome to our program Mr. physician21.
Physician21: Thank you, Sir.
Interviewer: In your opinion, why is there a need for a model of disease?
Physician21: Well. There are indeed many views of disease that came up with the understanding of the disease process. In my new model I try to make use of all these views in one working model.
Interviewer: Great, then, let’s get closer to your model!
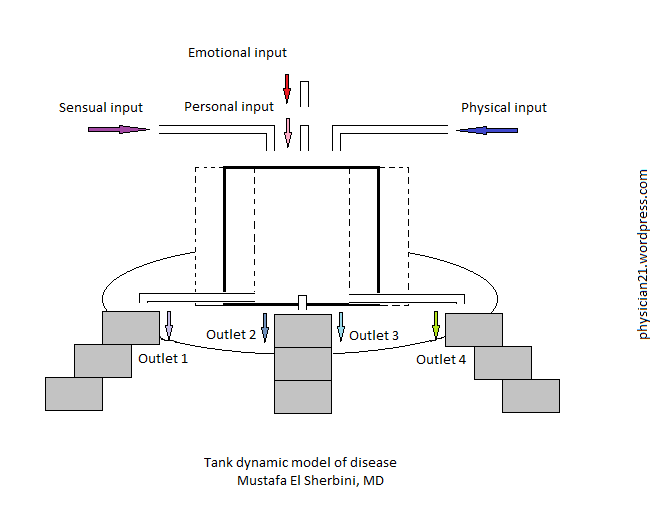
Physician21: The model considers the environmental variables, the physical elements including food and drinks, the emotional experiences and the personality.
Interviewer: Yes. Those 4 components are known to contribute to human health state. So, what is new in your model?
Physician21: The model assumes that everybody has a residual disease state at any point of time, and the disease is just an outbreak point of an already existing and ongoing process. The point is that one should take care to set that residual disease state as low as possible, so that such outbreaks would occur very infrequently.
Interviewer: What examples would you tell us in this respect?
Physician21: For example, the negative feelings such as hate and jealous, these are very inappropriate for one’s health. In the Islamic rituals, it is recommended for a sick person to give out money as alms or charity, and it is believed that this would directly or indirectly help cure the sick. This act can be understood in my model such that the act of giving money to the needy would creat a positive feeling or positive energy for the sick and the surrounding persons that would boost their readiness for cure and resolution.
Interviewer: So, your model emphasizes that health state comes from within the person, and encourages everybody to take care of naturally given health elements in those 4 discrete categories: environment, matter, emotions and personality.
Physician21: Yes, true. The process is very interesting and intricate. Everybody owns the keys for good health, just on realizing their proper use. The way one walks, talks, and behaves, all that speak either for or against the health state. So, one should be careful.
Interviewer: So, the progression of a disease state is largely controllable especially at its early beginning.
Physician21: Yes, of course.
Interviewer: You talked about positive and negative energy. is it the energy ‘halo’ of the body?
Physician21: Yes. According to physics matter can ultimately change to energy and both are interchangeable. Pictures, actions, meanings, thoughts, colors, sounds, clothes, objects and food can all take part in outshaping of the energy environment and feelings and, thus, health of the person.
Interviewer: Good. What about the biological and physio-chemical agents as disease causes in your model?
Physician21: These are called extraneous factors that may cause harm or not according to the basal disease or readiness of the person. So, they are not in the center of disease process in our model.
Interviewer: Thank you very much, Mr. physician21 for this great information.
Physician21: You are welcome, Sir. Thank you very much.
Tag: clinic
Tank dynamic model of disease
In science it is usual for a certain entity or process to describe a model that may describe, explain, or predict facts and phenomena concerning that natural entity or process. In this regard the disease process may not be an exception. Indeed, the disease process, and thence the cure method, is being regarded from several aspects that would complement each other in understanding the diseases and providing cure measures, or individually suggest an opinion that is not readily usable by other medical views.
In this essay, I shall present my own perception of the disease process with new name coinage, the tank dynamic model of disease.
1) What is a disease?
The disease is a deranged health status that can be subjective (addressed only by the person) or objective (addressed by the surrounding persons).
2) What are the basic common pillars of the disease?
The disease should have: 1- a complaint (picture), 2- a time onset, 3- a pattern, 4- a natural course, 5- opponents and proponents (things that oppose or favour), 6- cause(s), and 7- treatment(s).
3) What are the assumptions of this model of disease?
1. The disease is a dynamic process.
2. Everybody has a basal disease state at any point of time.
3. The matter and energy of an individual are interchangeable as explained by physics.
4. The disease ensues as an over flow of an already present and ongoing process in which a few unitary disease elements are in play, with or without the incidental superimposing an extraneous factor (a biological or a chemio–physical incident).
5. The unitary disease elements include: 1- sensual elements: environmental conditions and landscape, 2- emotional elements: fear, grave, happiness, hate, etc., 3- physical elements: exhaustion, tiredness, thirst, hunger, satiety, over- satiety, cold, hot, physical sexual overflood (stagnation), and 4- personal elements: shyness, honesty, intelligence (theoretical and social), sensitivity, etc.
6- The treatment of a disease condition comprises the timely and ordered measures according to the underlying contributing disease elements.
4) How is the disease process viewed in this model?
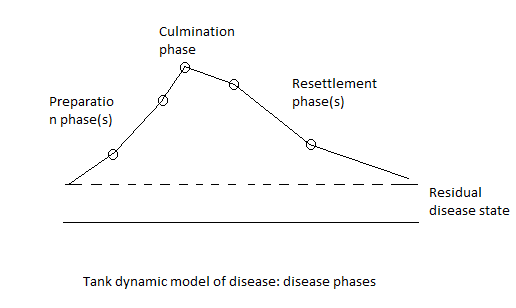
The disease has 3 phases: 1- preparatory phase, 2- shock or culmination phase, and 3- resettlement phase.
The disease may have one of 3 forms: 1- disease with mainly extraneous factor determinations (e.g. fever, malaise), 2- disease with mainly general physical phenomena (fatigue, fainting, hypertension, etc.), 3- disease with mainly neuropsychic phenomena (anxiety, depression, obsession, …).
5) How do the disease elements work?
The disease elements may work in triplets for many disease processes. Other more complicated disease elements’ contribution may be present.
6) Which diseases would you choose to explain as examples?
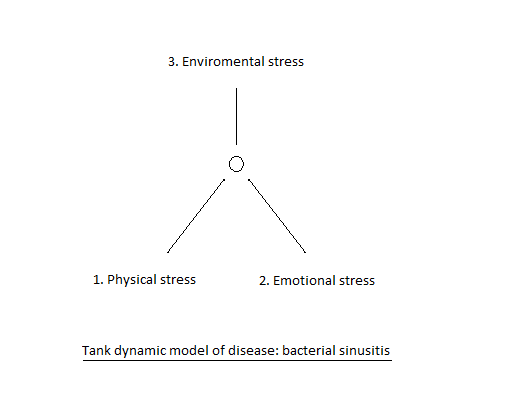
1. Bacterial sinusitis:
The disease elements can be: 1- physical stress (exhaustion, little food, little drinks, inability to properly clean the nose; e.g. lacking the hygiene paper tissue), 2- emotional feeling of pressure and shortage, and 3- environmental stress (hot, cold or dust).
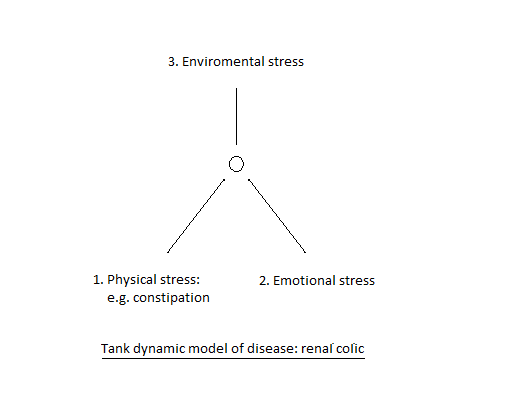
2. Renal colic
3. Fainting
Human health and filling in the gaps
There are seemingly no clear boundaries between health and disease of humans. From one side the judgement of one’s health may be subjective, and from the other side the feeling of being healthy or sick may be intermingled in the different parts of the same day. One of the most impactful insights in medical sciences is to find the appropriate definition of health and disease statuses. The definition of health laid by the World Health Organization states health as “the state of complete physical, mental and social well-being, and not merely the absence of disease and infirmity.” Apparently and in practical terms no one on Earth would fit to the WHO definition as being a healthy human.
The human health, being the sum of several biological components or entities, should not be regarded apart from its inherent dynamic nature. It can, therefore, be considered and expressed in hand of mathematical probability estimation. The human health may be, accordingly, defined as the state of satisfactory physical, mental and social showing in average life conditions with or without auxiliary means in terms of lifestyle and/or medical treatment. Therefore, in light of this definition while health state judgment may be individually tailored and appreciated, the presence or absence of certain physical or psychological disease state would be regarded as a constitutional health element for every individual. For the delineation of such constitutional health elements, physicians and other health scientists may succeed in writing down all known conditions (or diseases) with their different possible classifications.
Such dynamic nature of human health should give a red alarm to physicians not to make statements on one’s health based only on some data in limited clinical sessions or visits. In many cases, closer observation and more rigorous data collection may be needed before the health state of an individual can be judged.
On handling certain health condition, the natural body resources and compensatory reserves (so-called natural healing power) should not be overseen, but rather boosted and encouraged. In other words, the medicines; if they are clearly indicated, should be given prudently so that such natural resources and reserves would still be desirably in action. The benefits of such prudent medical conduct include: 1) preservation and boosting of natural healing would ensure permanent or durable cure and reflect positively on longevity, 2) giving less medicines with less chances for side-effects and with lower cost, and 3) deliberate ‘undertreatment’, i.e. prudent treatment, would allow easy-to-follow life style and help avoid iatrogenic (of doctor origin) and accidental overdosing.
The clinical medicine logic
The physician works in a large frame of 3 pillars: the preventive medicine, the diagnostic medicine and the curative medicine. From a broad practical view the physician’s job is mainly in the curative medicine pillar.
The clinical (curative) medicine logics may be thought of as:
1- Adjunctive medicine
– analgesic, sedative, anxiolytic
– Mood modifiers
– Psychoactive agents
2- Casual medicine
– surgery
– invasive diagnostic and therapeutic interventions
3- Regular medicine
– nutrition
– common nonspecific agents: laxative, purgative, emollient, carminative
– specific medical agents
– antibiotics and antimicrobials
– anticancer agents
The physician’s guide

The physician’s guide is an indispensible tool to summarize basic medical and clinical knowledge and experiences. It should be concise, easily demonstrable, regularly updated and greatly physician-specified (self made).
Here is a personal view of such important medical tool.
The Hippocratic Oath
Section 1: normal values (pediatrics: growth milestones or curves, caloric and fluid requirements and calculations; CBC; hemoglobin electrophoresis; plasma electrophoresis; liver function; kidney function; urine; stools; semen; hormones; electrolytes; arterial boold gases; and ECG findings).
Section 2: preparation-oriented drug index (topical formulas: skin, eye, ear, and nose; tonics and food supplements; antimicrobials: antiseptic, antibiotic, antifungal, antiprotozoal, and antihelimenthics; analgesics and antipyretics; antihistaminics; corticosteroids; skeletal muscle relaxants; antispasmodics; antihypertensives and cardiac agents; hemostatics, hypoglycemics; neuropsychiatric agents (sedatives and hypnotics, anticonvulsants, brain stimulants, antidepressants, antiparkinsonians); and beauty preparations (shampoos, cosmetics, soaps, etc.).
Sections 3: natural foods and herbs – sorted alphabetically – and their uses (basilica, chamomile, garlic, green tea, onion, thyme, etc.).
Section 4: medicines’ doses and instructions tables (neonate, child, and adult).
Section 5: crude models of medical prescriptions (orthopedic, eye, ear, nasopharyngeal, dermal, gynecologic, oral, cardiac, digestive, liver, renal, respiratory, and neuropsychiatry).
Section 6: medical algorithms (pediatrics: infant of diabetic mother, muconial aspiration, low birth weight, prematurity, neonatal jaundice, respiratory distress, etc.; adults: HTN, DM, bronchial asthma, cardiac asthma, DVT, diabetic ketoacidosis, hypoglycemia, stroke, etc.).
The ten golden rules in rescuing the (medically) troubled

Situations in which medical care or advice should be provided vary considerably as regard place, time and the extent of the medical problem, i.e. patient’s state as regard consciousness, cooperation, presence of patient’s relatives, etc.
Here are 10 rules that I wish to conclude from my experience in the clinical field.
1- The sense of being attended: the health care provider should stress and make sure that the patient perceives that a good medical care is being present. This would be achieved by speaking gently and confidently with the patient and/ or with the relatives. The doctor may state clearly that he/ she would have no problem to see the patient for free when the patient’s condition money-wise is not favorable. The doctor should be cautious as much as possible to protect the patient from possible negligence by his/ her relatives. In case of a patient with perturbed consciousness the doctor would call the patient by his/ her name (if known) and hold the patient hand warmly.
2- Resort and handing: the doctor would have preliminary assessment of the medical problem, and recalls his/ her knowledge and may need to find some source as a book or contact a colleague for consultation. The doctor may have to urge for a referral to a more experienced doctor.
3- Fulfilling continuum: the doctor may inspire that human body is one continuum with dynamically operating modes and proportionately distributed components. This should be very useful in determining the dose, rate, and intervals of the medicines to be used.
4- Hierarchical approach: the management plan should be almost clear from the beginning. The management should assume a hierarchical concept as regard the relevance of interventions/medicines to one another from one side and to the human body function from the other side. It should start from natural means to encourage the self-curing power in the patient, e.g. warming the patient, changing posture, etc., and proceeding from a less invasive to more invasive.
5- Multi-footed treatment: this means that using more than one point or target in the treatment, if allowable, would help reach a more smooth response with less likelihood of misfortune. This integrated approach would allow less and more tolerable medicine doses.
6- Proof tracking: this means that on following certain treatment the doctor keeps an open eye checking back and forth for the consistency and appropriateness of a given step in the management for a possible need to change the treatment plan.
7- Case cliché: by the time the medical condition is being resolved the doctor should formulate a clear definition of the case (diagnosis) and inform the patient or the relative(s), orally and/ or in writing.
8- A Gift-outcome-art: this means that the outcome of the medical care is quite unforeseeable. Here, the outcome is usually expressed as percentages or probabilities and not as a definitely individualized result.
9- Non obligation: the medical care should not bear any obligation from both patient’s and doctor’s side.
10- Medical ethics: the doctor should be aware of and fulfilling the medical ethics applicable to the particular medical problem being managed.
